Last updated on March 3rd, 2020 at 04:24 pm
Modafinil is a wakefulness-promoting nootropic that is widely regarded as the best alternative to adderall. Modafinil provides nearly all the benefits of adderall, albeit to a weaker degree, but without the side effects like anxiety, tunnel vision and tachycardia.
| Overview | |
|---|---|
| Also Known As | Provigil, Alertec, Modavigil, Modiodal, Modalert |
| Type | Pharmaceutical Stimulant |
| Main benefits |
|
| Synergistic with |
|
| Typical route | Oral |
| Typical dose | 200 mg |
| Typically taken | Acutely |
| Half-life | 12-15 hours[94][97] |
| Mechanism of action | Primary: Dopaminergic Secondary: Affects noradrenaline, serotonin, glutamate, GABA, histamine, and orexin |
Table of Contents
Summary
Modafinil is unique in that it induces wakefulness without causing stimulation. This is in contrast to classic stimulants like caffeine, adderall, and ritalin, which provide wakefulness as a result of stimulation. Its use has become more and more prevalent because of its relatively benign profile. It provides many benefits with little to no side effects. Modafinil is used to enhance cognition, improve ADHD, improve cognition during sleep-deprivation, augment antidepressants, and as a mood enhancer.
Its main mechanism of action is unknown but it is known to act as a potent, but weak dopamine reuptake inhibitor. It’s also an alpha-1 adrenoceptor agonist.
Benefits of modafinil
Summary of benefits
| Condition | Effect | Dosage | Subjects |
|---|---|---|---|
| Cognition | Enhanced: working memory, recognition memory, sustained attention, and other cognitive functions | 100 - 200 mg |
|
| ADHD | Strong decrease in symptoms; equivalent to that of dextroamphetamine | 100 - 425 mg |
|
| Depression |
| 100 - 400 mg |
|
| Fatigue | Strong decrease | 100 - 300 mg |
|
| Motivation | Increased task enjoyment | 200 mg | Healthy adults Rats |
| Mood | Improvement | 400 mg | Depressed adults |
| Prolactin | Decrease | 200 mg | Healthy males |
| Cortisol | No change | 300 mg twice daily | Healthy males |
| Growth hormone | No change | 300 mg twice daily | Healthy males |
| Melatonin | No change | 300 mg twice daily | Healthy males |
Cognition
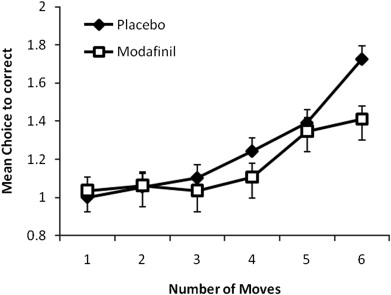
In three studies, researchers found that non-sleep deprived healthy subjects given modafinil had enhanced task enjoyment and performance on several cognitive tests of planning and working memory, but had no improvements in paired associates learning.[1][8][46] Another study employing 33 subjects found those given 200 mg learned a new language faster than those given placebo.[2] Though, this study found no improvement in working memory. In 12 healthy males, at 300 mg, it was found to decrease the number of errors in the One-Touch Stockings of Cambridge test, which measures executive function, spatial planning, and working memory.[44]
Several studies have shown that modafinil does not improve cognition in healthy adults.[3][4][5] However, some studies do show some enhancements in verbal recall, short-term visual recognition memory and improvement in a simple colour naming of dots. Two of these studies suggest that modafinil’s cognitive benefits may be limited to those with a low IQ or low-performing individuals.[4][46] This is backed by another study which showed it enhanced cognition in those suffering from ADHD with “improvements on tests of short-term memory span, visual memory, spatial planning, and stop-signal motor inhibition” and sustained attention span, but not in healthy individuals.[6]
In contrast, another study found improvements in focus and accuracy in healthy adults, but only in demanding tasks.[7] Modafinil appears to be a viable alternative to adderall, ritalin, and other medications for ADHD. It improves attention span, decreases errors in demanding tasks, and even reduces impulsiveness.[8][49]
Modafinil was able to increase cognitive performance in working memory and learning in 11 healthy non-sleep deprived adults and its effects were comparable to that of dextroamphetamine.[63]
In summary, modafinil’s effects on cognition are not very reliable. There appears to be an apparent benefit to those suffering from ADHD, low IQ,or other cognitive deficits. However, in regards to healthy adults, the results are mixed with some studies showing enhanced cognition and others showing little to no change.
Attention deficit hyperactivity disorder (ADHD)
Aside from improving general cognitive processes in those with ADHD, modafinil was found to successfully treat ADHD itself. In a study with otherwise healthy adults, approximately 207 mg +/- 85 was found to be comparable to approximately 22 mg +/- 9 of dextroamphetamine in treating ADHD.[64]
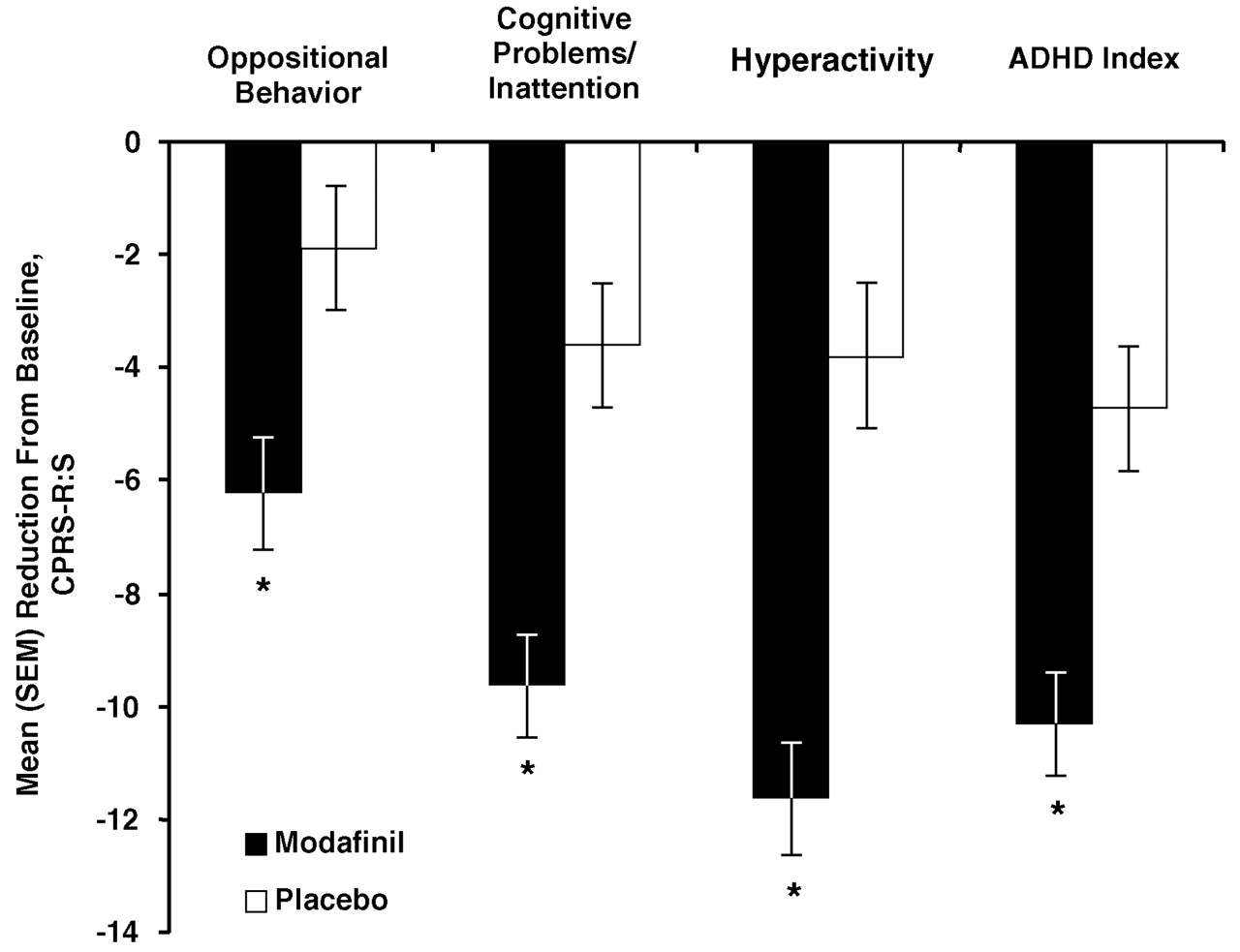
In children and adolescents, several studies have shown modafinil to be effective in treating ADHD. It had minimal side-effects and was well-tolerated in two different 9-week double-blind studies.[65][66] Both studies found it to significantly improve ADHD symptoms, both at school and at home. Likewise, a different study found a significant reduction in ADHD Symptoms at school following 6 weeks of treatment.[67] One more study also found a significant reduction in ADHD symptoms at school and home, but abrupt discontinuation following 2 weeks of treatment did not cause a rebound in ADHD symptoms nor cause withdrawal symptoms.[68]
Another study using children and adolescents found a once-daily dose of 300 mg to be more effective than a split-dose. Those taking divided-doses had inconsistent improvements in ADHD symptoms whereas those taking once-daily had significant and consistent improvements.[69]
Modafinil is a viable treatment for ADHD in adults, adolescents and children. It significantly improves symptoms of ADHD and is generally well-tolerated. A once-daily dose is more effective than split-doses.
Sleep deprivation
Sleep deprivation is well-known to impair performance and cause several cognitive deficits.[9][10][11][12] Modafinil is one of many substances that can reduce the negative effects of sleep deprivation on cognition, the others being caffeine and stimulants such as adderall. One study found that modafinil given to healthy adults restored objective performance and alertness during sleep deprivation with few side effects.[13] However, another study found that while it maintained performance and alertness during sleep deprivation, its effects were no more stronger than that of caffeine.[14]
One study employing 6 young males (20 – 24 years old) found a dose-dependent benefit on cognitive performance during 64 hours of sleep deprivation with 300 mg total being the most effective.[16] However, it was dosed 3 times a day at 8-hour intervals as opposed to taking it at once in the morning. This is rather unusual and it’s not clear why the study employed such a dosing regimen given modafinil’s 12-15 hour half-life. Nonetheless, at 300 mg total (100 mg every 8 hours), it was found to maintain cognitive performance at or near baseline value. At 150 mg (50 mg every 8 hours), it only provided some maintenance on performance and at 50 mg (16.7 mg every 8 hours) the effect was no more different than that of placebo.
Comparing amphetamine to modafinil, at least one study found both 20 mg of d-amphetamine and 300 mg of modafinil to improve mood, fatigue, sleepiness, and cognitive performance following 64 hours of sleep-deprivation with no differences between the two.[18] However, subjects taking modafinil experienced fewer side-effects than those taking d-amphetamine. Body temperatures in both groups were increased or maintained compared to the placebo group.
In short, modafinil appears to reliably reduce the detrimental effects of sleep deprivation on cognition with little to no side-effects. Furthermore, it is able to reduce the need for longer sleep following sleep deprivation.[17] This makes modafinil a great alternative to caffeine and amphetamines for counteracting the effects of sleep-deprivation. However, it is unable to prevent detriments in cognitive function following long periods of sleep deprivation.[49] As such, it is imperative that one get adequate sleep when possible.
Motivation
Healthy adults given 200 mg experienced an increase in task enjoyment.[1] In rats, it was found to increase motivation by increasing dopaminergic activity.[19] Indeed, the same effect is seen in humans where it increases dopamine in the nucleus accumbens.[20][62] This part of the brain plays a significant role in motivation, pleasure, and reward. This reinforces the idea that modafinil can improve motivation in humans. Further studies are needed to verify this finding.
Mood
Healthy adults given 400 mg of modafinil experienced an increase in general mood and a significant increase in positive thinking and emotions.[21]
Depression and fatigue
In patients with depression, it was found to improve mood, reduce fatigue, and relieve excessive sleepiness.[22] It appears to augment SSRI-treatment therapy and increases the chances of achieving remission. Several studies have shown significant improvements in fatigue and sleepiness when SSRI-treatment is augmented with modafinil.[23][24][25][26][27][28][29][30][52] In these studies it was well-tolerated and had minimal side-effects. One study even showed an increase in response-speed on top of an enhancement of the antidepressant effects.[24]
Most of these studies used 100 to 200 mg of modafinil taken once a day. Another study found modafinil to augment not only SSRIs, but also venlafaxine (Effexor), mirtazapine (Remeron), and tricyclic antidepressants. [70] Doses ranged from 100 to 400 mg daily. Treatment lead to a remission rate of 43%.
Other studies in bipolar-depression patients also show significant improvements in depressive symptoms with no increased risk of mania.[30][31]
At least one study has found modafinil by itself to be effective for atypical depression. Doses ranged from 100 mg to 400 mg, depending on the patient’s tolerability.[34]
It also appears to be effective for Seasonal Affective Disorder according to one study that used 100 mg or 200 mg taken twice daily.[51]
There are 3 case reports of modafinil safely augmenting MAOI antidepressants with no signs of tolerance.[100] One case report involves a 58 year old man who lacked energy, was anhedonic, hypersomnic, had slowed thoughts and negative thoughts. Many antidepressants were tried, but to no avail. Finally, he achieved partial remission with the initiation of transdermal selegiline and was moved up to a maximum of 24 mg. Despite selegiline being a selective MAO-B inhibitor, at high doses it significantly inhibits MAO-A in addition to MAO-B. Tianeptine was used in combination with selegiline but lacked efficacy and was discontinued, though it did not have any adverse effects. However, with the addition of 200 mg of modafinil the patient achieved complete remission and remained in remission for over 24 months after his last follow up.
Another case report involves a 55 year old man who also tried many antidepressants before being placed on transdermal selegiline at 12 mg daily. This improved his energy, but did not help his concentration problems nor his problem of becoming easily fatigued. He achieved complete remission with the addition of 400 mg of modafinil and did not have any significant side effects. Furthermore, he discontinued selegiline after 6 months, but remained in remission for over 24 months after his follow up.
The last case report involves a 60 year old woman who has a long history of depression. She was taking 120 mg of tranylcypromine, 37.5 mg tianeptine, and an atypical antipsychotic. Most of her symptoms were controlled, but she lacked energy. The addition of 400 mg of modafinil reduced her fatigue and had no significant side effects. She remained in partial remission 2 years after starting this regimen.
There is strong evidence to support the use of modafinil as an augmentation strategy in the treatment of depression, especially with SSRIs. It also appears to be effective and safe in bipolar-depression and does not increase the risk of developing mania
Hormones
Healthy males in two separate studies given either 200 mg of modafinil or 400 mg experienced a decrease in prolactin levels.[47][50] With regards to plasma cortisol, growth hormone, and melatonin, 300 mg of modafinil administered twice in a 36 hour sleep-deprivation session failed to alter plasma hormone levels. In non-sleep deprived healthy males at 400 mg, it does not affect plasma hormone levels of growth hormone and thyroid-stimulating hormone (TSH).[50]
Stimulation
A double-blind study using 300 mg of caffeine, 15 mg of dextroamphetamine, and 300 mg of modafinil in 16 healthy subjects found modafinil to subjectively feel similar to caffeine. As in, it was free from side-effects associated with traditional stimulants.[53][54][101]
Two studies employing 100 mg to 200 mg of modafinil found a significant decrease in cancer-related fatigue.[55][56] In contrast, a larger double-blind study consisting of 208 cancer patients found no significant decrease in cancer-related fatigue.[57]
HIV
Two small studies have shown modafinil to decrease HIV-related fatigue and improve cognitive functions, including verbal memory and executive function.[58][59] A larger double-blind study employing 115 HIV-positive patients found a significant decrease in fatigue and depressive symptoms with no signs of tolerance after 6 months of treatment.[60]
Mechanism of action
Humans
| Neurotransmitter | Change | Mechanism | Effect | Dosage |
|---|---|---|---|---|
| Dopamine | Increase in dopamine levels | Inhibition of dopamine reuptake | Increased wakefulness | 200 mg - 400 mg |
| Noradrenaline | Increased activity | Agonism of Alpha-1 adrenergic receptor |
| 200 mg |
| Histamine | Increased metabolite levels | Unknown | Increased wakefulness | N/A |
Dopamine
How modafinil works is largely a mystery. Though, it is known to increase dopamine in the nucleus accumbens and inhibit the dopamine transporter (DAT), but it does so without being addictive.[36][45] In contrast, classic DAT inhibitors like cocaine are well-known for producing euphoria and causing addiction. What’s more is when cocaine and modafinil are administered together, cocaine’s positive effects are significantly blunted.[37][38] Interestingly, two studies have found modafinil to treat cocaine dependence. It reduced cravings and increased the likelihood of cocaine abstinence. One study employed 300 mg daily and the other 400 mg.[39][40] This reinforces the idea that modafinil increases dopamine in the brain by a mechanism similar to that of cocaine.
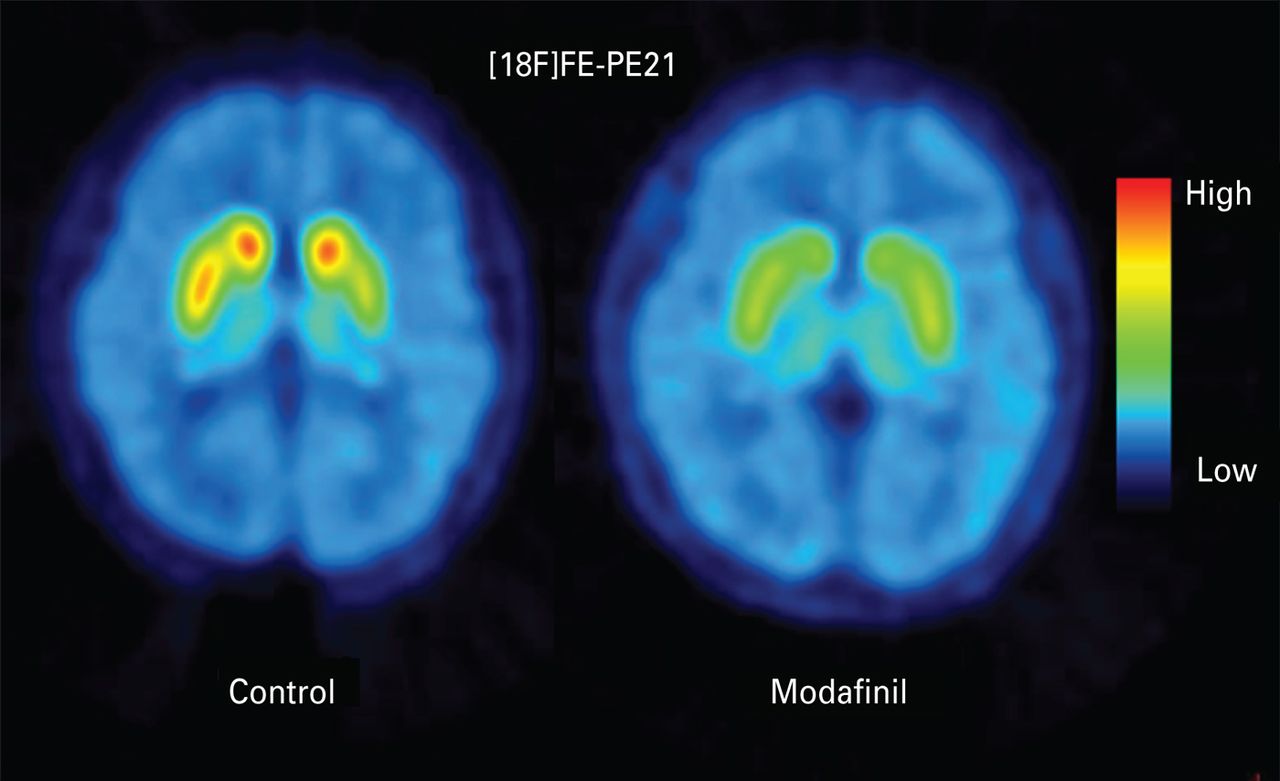
In healthy volunteers, modafinil was able to inhibit 51.4% of dopamine transporters (DAT) in the striatum at 200 mg and 56.9% at 300 mg. It also increased dopamine in the nucleus accumbens with 200 mg occupying 51.5% of DAT and 300 mg occupying 57.7%. The same study suggested that modafinil is almost as potent as methylphenidate (ritalin) in occupying DAT.[62]
Modafinil also reduces prolactin in healthy humans via a dopaminergic mechanism.[47]
There is research to suggest those with different types of COMT genes respond differently to modafinil.[61] Those with the Val/Val genotype supposedly have lower dopamine levels than those with the Met/Met genotype. In a study using sleep-deprived healthy volunteers, Val/Val individuals responded very well to 100 mg taken twice while those with Met/Met hardly had any effect. Nonetheless, this study should be taken with a grain of salt as modafinil’s mechanisms are quite complex. Furthermore, there are several anecdotes in which users without the Val/Val genotype responded positively to modafinil. And there are even some users with the Val/Val genotype who did not respond at all. Further studies are needed to confirm these findings.
There is strong evidence modafinil inhibits the reuptake of dopamine via the dopamine transporter. It increases dopamine in the striatum, nucleus accumbens, and other parts of the brain. However, it is unclear if this increase is solely responsible for its wakefulness-properties.
Noradrenaline
At least 4 studies have shown modafinil to increase noradrenergic activity, with two suggesting it acts as a central alpha-1 adrenoceptor agonist and the others suggesting it increases noradrenergic activity in the Locus Coeruleus (LC).[41][42][43][44] The LC is a part of the brainstem that produces most of the brain’s noradrenaline. It is involved in wakefulness, memory and attention, executive functions, emotions, and neuroplasticity.
The alpha-1 adrenoceptors may be partially responsible for modafinil’s nootropic effect. Antagonism of this receptor blocks modafinil’s ability to reduce errors on the One-Touch Stockings of Cambridge test.[44] This test measures executive function, spatial planning, and working memory. It is not clear which of these cognitive functions is diminished by antagonism of the alpha-1 adrenoceptor as they are all important for the test. However, one study found modafinil to subtly enhance working memory via a noradrenergic mechanism in the prefrontal cortex.[46] This suggests that the beneficial effects of modafinil on working memory involves a noradrenergic mechanism.
No study has shown modafinil to activate the alpha-1 adrenoceptors outside the central nervous system (CNS). This could, in part, explain the relative lack of stimulant-like side effects.
Modafinil is confirmed to agonize the central alpha-1 adrenoceptors in humans. At least some of its nootropic effects are mediated by a noradrenergic mechanism.
Histamine
One study employing the use of tiprolisant, an H3 inverse-agonist, found modafinil to augment its effects. Moreover, in mice it was shown to increase tele-methylhistamine, a histamine metabolite, suggesting it increased histamine release. The researchers did not conclude whether modafinil also increased histamine in humans but did suggest it may act on the histaminergic system.
Animals and lab studies
In rats and mice, modafinil’s mechanism of action appears to be quite complex. It has varying effects on dopamine, glutamate, serotonin, GABA, histamine, acetylcholine, and orexin.
| Neurotransmitter | Change | Mechanism | Effects | Subjects |
|---|---|---|---|---|
| Dopamine | Increased levels |
| Increased wakefulness |
|
| Norepinephrine | Increased levels |
| Increased wakefulness |
|
| GABA |
|
| May be involved in wakefulness |
|
| Glutamate | Increased levels | GABAergic mechanism | Unknown | Rats |
| Histamine | Increased activity |
| Increased wakefulness | Mice |
| Orexin | Increased activity | Increased histamine release |
| Mice |
| Serotonin (5-HT) |
| Increased release in the prefrontal cortex | Unknown |
|
Dopamine
Many studies have shown dopamine plays a pivotal role in modafinil’s’ mechanism of action. One such study found it to be ineffective in mice lacking the dopamine transporter.[71] Another study found the dopaminergic D1 and D2 receptors to be critical for the wakefulness properties of modafinil.[72] Furthermore, quinpirole, a dopamine autoreceptor agonist, was found to blunt modafinil’s wakefulness-promoting efficacy in mice.[73]
Similarly to amphetamine, dopamine release is increased in the striatum of rats following a single dose.[74] However, modafinil was much less potent at releasing dopamine than amphetamine. Another study, also using rats, found that an increase in dopamine and serotonin release is responsible for the initial waking effect while increased noradrenaline release maintains it.[75]
At least some of the increase in dopamine release is mediated by altered GABA activity. Baclofen, a GABAB receptor agonist, augments modafinil’s action on dopamine release.[84]
In rhesus monkeys, it was found to bind to the dopamine transporter. Moreover, it was also found to bind to the human dopamine transporter (DAT) with strong affinity in-vitro.[76]
In contrast to these findings, one study on rats found modafinil to have no effect on the firing rate of dopaminergic neurons and concluded that its wakefulness-properties are not mediated by a catecholaminergic mechanism.[77]
Noradrenaline
Cats given modafinil experienced a dose-dependent increase in wakefulness. When combined with adrenergic antagonists, modafinil’s arousal effect was significantly decreased. But, when combined with a catecholamine synthesis inhibitor, its effects were slightly reduced in duration. The study suggested its mechanism of action was due to an enhancement of alpha-1 and beta-receptor activity.[78] Indeed, in mice and monkeys, its effects have been linked to stimulation of central alpha-1 receptors.[79] Interestingly, modafinil appears to selectively agonize the alpha-1 adrenoceptors in the CNS leaving the peripheral receptors untouched. The implications of which are not fully known, but can explain the relative lack of stimulant-like side-effects seen in humans.
Noradrenaline levels in the hypothalamus are significantly increased in rats following a single dose.[75]
In an in-vitro study, it was found to bind to the human norepinephrine transporter (NET) with moderate affinity.[76]
GABA
Modafinil appears to reliably reduce GABA levels in rats, mice and guinea pigs. Moreover, its decreases GABA release via an indirect mechanism involving serotonin, dopamine and noradrenaline. Antagonism of the serotonin type 2 (5-HT2) prevents modafinil’s ability to reduce GABA release.[80] And antagonism of the 5-HT3 receptor blunts the reduction of GABA.[81][86] Guinea pigs given 6-hydroxydopamine, a neurotoxin that kills dopaminergic and noradrenergic neurons, did not experience a decrease in GABA levels following modafinil administration.[82] Serotonin-depleted guinea pigs and rats not only experienced no reduction in GABA, but had an increase in GABA and noradrenaline.[83]
A GABAergic mechanism is at least partially responsible for the increase in dopamine release as guinea pigs given a GABAB receptor antagonist, a GABAA receptor agonist, or a GABA reuptake inhibitor did not experience an increase in dopamine release.[84]
No effect was seen on GABA synthesis in an ex-vivo and in-vitro study using the rat hypothalamus.[85]
Glutamate
In rats, modafinil is able to increase glutamate levels in the rat brain via a GABAergic mechanism. Agonism of the GABAA receptor blunts the increase in glutamate levels whereas antagonism enhances it.[86]
No effect was seen on glutamate synthesis in an ex-vivo and in-vitro study using the rat hypothalamus.[85]
Histamine
Two different studies have shown modafinil to increase histamine release, but not directly. When it was injected directly into an area of the brain with histaminergic neurons, it failed to alter histamine release.[87] Rather, it appears modafinil is able to increase histamine release via an interaction with orexinergic neurons.[88] One of the studies found it to increase histamine release to 150% of baseline, though the dose was rather large at 150 mg/kg for which the human equivalent dose (HED) is about 24 mg/kg.[87]
A study using modafinil and tiprolisant, an inverse H3 agonist, found modafinil to modestly increase tele-methylhistamine levels, a metabolite of histamine.[89]
Orexin
Aside from increasing histamine release, orexin neurons are not needed for the wakefulness properties of modafinil. In fact, orexin-null mice had significantly longer wakefulness times than did their wild-type counterparts.[90]
Serotonin
An in-vitro study found modafinil to weakly bind to the human serotonin transporter (SERT).[76]
Acetylcholine
No effect was seen on acetylcholine levels in rats.
Side effects
Much like caffeine, modafinil has a very benign side-effect profile. It does not seem to cause a drugged-up feeling like the classic stimulants adderall and ritalin. It also does not seem to have any prominent side-effects, unlike stimulants which are almost always associated with decreased appetite, racing heart, and increased anxiety. The most common side-effect is that it lasts too long. While some may argue this is not a side-effect, by definition a side-effect is an unintended effect of a drug. In modafinil’s case, because it lasts 12-15 hours it can affect some people’s sleep. Some may have trouble sleeping while taking modafinil, even if they take it in the morning.
One study found this to be true with modafinil impairing post-recovery sleep following sleep-deprivation.[13] However, several other studies have found no such detriment to recovery sleep.[15][92][93] On the contrary, one study found it to decrease the need for a longer sleep following sleep deprivation and another found it to increase subjective sleep quality.[17][92]
Regardless, there are many ways to counteract this side effect. The simplest way is to reduce the dosage. Cutting the tablet in half can help to mitigate this side effect, but may decrease the benefits as well. Another way is to take supplements and nootropics for sleep. Melatonin, phenibut, and L-Theanine are all excellent choices for inducing relaxation and sleep. However, phenibut should only be used acutely. Chronic use is not recommended as it can be addictive.
Another common side effect of modafinil is increased itchiness. Because it increases histamine, it can worsen allergies and induce itchiness. It can also cause a very rare condition called Stevens–Johnson syndrome. However, the odds of this happening are quite slim.
Some studies on humans have found modafinil to increase anxiety and aggressive mood factors.[21][35]
A systematic review found modafinil to impair creativity.[91]
Tolerance
Modafinil at 400 mg daily was found to be effective at treating excessive daytime sleepiness for up to 40 weeks.[95] No tolerance was observed. However, while most studies don’t show any signs of tolerance, there are many anecdotes that modafinil’s effects weaken or even disappear over time. Many users notice a particular smell in their urine a number of hours after taking it. And when these users take modafinil over several days or weeks, they notice their urine starts to smell much earlier than usual. This suggests that modafinil is being metabolized at a faster rate.
Indeed, there is some evidence to support this notion. Modafinil is an inducer of the CYP3A4 enzyme or in other words, it increases the activity of the CYP3A4 enzyme. This enzyme is one of many that metabolizes modafinil. However, it seems modafinil is mainly metabolized by amide hydrolysis.[94] It’s unlikely that induction of the CYP3A4 enzyme is solely responsible for this effect.
HIV-positive patients taking up to 200 mg of modafinil a day for 6 months did not experience a reduction in the fatigue-reducing and antidepressant-like benefits.[60]
In terms of its antidepressant-like effects, no tolerance was seen in 3 case reports following 24 months after initiation of modafinil.[100]
Regardless of these findings, cycling is recommended to maintain its full effects in healthy users.
Synergies
Caffeine
Dopamine seems to be fundamental to modafinil’s mechanism of action. Mice lacking the dopamine transporter do not experience increased wakefulness upon administration of modafinil. In humans, modafinil increases dopamine in the nucleus accumbens and the striatum and caffeine increases the density of the striatal dopamine D2 and D3 receptors. The nucleus accumbens and the striatum are involved in motivation, pleasure, reward, and reward perception. Based on this, caffeine should synergize perfectly with modafinil to increase motivation and other beneficial effects. However, it can also decrease motivation and focus through overstimulation. Because of this, it is important to keep the caffeine dose low and to take L-Theanine in addition to caffeine and modafinil.
Example of a stack:
- 200 mg Modafinil
- 100 mg – 200 mg Caffeine
- 100 mg – 200 mg L-Theanine
Selegiline
Selegiline is an irreversible MAO-B inhibitor used to treat Parkinson’s disease. Monoamine oxidase type B (MAO-B) is an enzyme found in the brain and the body that metabolizes dopamine and phenethylamine (PEA). PEA is an endogenous amphetamine-like compound that releases dopamine and norepinephrine. Selegiline is well-known to increase striatal dopamine levels which as a result can enhance modafinil’s ability to increase motivation. However, selegiline is not recommended for new nootropic users because of its complexity. For one, selegiline needs at least 2 weeks before dopamine levels are increased to a significant degree. It also lasts quite a long time with some MAO-B enzymes remaining inhibited after a month of not taking selegiline.
It can also result in overstimulation in vulnerable individuals. If you already respond to modafinil then there is no need to take selegiline. If you don’t respond to it, or you only partially respond then you can consider adding in selegiline. But, a single dose won’t have any effect on modafinil. It needs to be taken chronically to achieve a significant effect.
Safety
Up to 600 mg, modafinil appears to be safe and beneficial without any major side effects. However, at 800 mg it significantly increases blood pressure and heart rate.[96]
A combination of 200 mg of modafinil and 10 mg of dextroamphetamine administered to healthy volunteers was well tolerated with no major side effects.[97]
No changes were seen in liver values when modafinil or armodafinil was administered to HIV-positive patients with hepatitis C.[58]
Modafinil and warfarin should not be taken together as modafinil inhibits CYP2C9, an enzyme that metabolizes warfarin. However, this was not the case in one study where 5 mg of warfarin was used with 400 mg of modafinil.[102] No changes in blood levels of warfarin were detected. Regardless, this is only one study and as such modafinil and warfarin should only be used with extreme caution.
Hypertension is rarely seen, but there is a case report of a 63 year old woman who developed high blood pressure after she started 300 mg of modafinil. The dosage was lowered to 100 mg daily, but to no avail. It was discontinued and replaced with 900 mg of adrafinil which also caused a significant rise in blood pressure. After discontinuing both, her blood pressure values normalized.[99]
A case report found the combined use of tranylcypromine (Parnate) parnate and modafinil in a narcoleptic patient was well-tolerated and effective in treating the patient’s narcoleptic symptoms.[98] Parnate is an old-generation classic MAOI. It is usually contradicted with many drugs for fear of serious cardiovascular complications. However, given modafinil’s lack of effects on the sympathetic nervous system, it should not increase the risk of hypertension. In addition, 2 case reports found a combination of high-dose transdermal selegiline and 200 mg and 400 mg of modafinil to be safe and well-tolerated.[100]
References
- Müller, U., Rowe, J. B., Rittman, T., Lewis, C., Robbins, T. W., & Sahakian, B. J. (2013). Effects of modafinil on non-verbal cognition, task enjoyment and creative thinking in healthy volunteers. Neuropharmacology, 64(5), 490–495.
- Gilleen, J., P.g. Michalopoulou, A. Reichenberg, R. Drake, T. Wykes, S.w. Lewis, and S. Kapur. “Modafinil Combined with Cognitive Training Is Associated with Improved Learning in Healthy Volunteers – A Randomised Controlled Trial.“European Neuropsychopharmacology 24.4 (2014): 529-39.
- Randall, Delia C., Aparna Viswanath, Punam Bharania, Sarah M. Elsabagh, David E. Hartley, John M. Shneerson, and Sandra E. File. “Does Modafinil Enhance Cognitive Performance in Young Volunteers Who Are Not Sleep-Deprived?” Journal of Clinical Psychopharmacology 25.2 (2005): 175-79
- Randall, Delia C., John M. Shneerson, and Sandra E. File. “Cognitive Effects of Modafinil in Student Volunteers May Depend on IQ.” Pharmacology Biochemistry and Behavior 82.1 (2005): 133-39
- Randall, Delia C., Nicola L. Fleck, John M. Shneerson, and Sandra E. File. “The Cognitive-enhancing Properties of Modafinil Are Limited in Non-sleep-deprived Middle-aged Volunteers.” Pharmacology Biochemistry and Behavior 77.3 (2004): 547-55
- Turner, Danielle C., Luke Clark, Jonathan Dowson, Trevor W. Robbins, and Barbara J. Sahakian. “Modafinil Improves Cognition and Response Inhibition in Adult Attention-deficit/hyperactivity Disorder.” Biological Psychiatry 55.10 (2004): 1031-040
- Marchant, Natalie L., Faddy Kamel, Kezia Echlin, John Grice, Mark Lewis, and Jennifer M. Rusted. “Modafinil Improves Rapid Shifts of Attention.”Psychopharmacology 202.1-3 (2008): 487-95
- Turner DC, Robbins TW, Clark L, Aron AR, Dowson J, Sahakian BJ. Cognitive enhancing effects of modafinil in healthy volunteers.Psychopharmacology (Berl). 2003 Jan;165(3):260-9. Epub 2002 Nov 1. PubMed PMID: 12417966
- Killgore, William D. S., and Mareen Weber. “Sleep Deprivation and Cognitive Performance.” Sleep Deprivation and Disease (2013): 209-29
- Killgore, William D.s. “Effects of Sleep Deprivation on Cognition.” Progress in Brain Research (2010): 105-29
- Griffith, Candice D., and Sankaran Mahadevan. “The Influence of Fatigue on Human Performance: Meta-analysis of Sleep Deprivation Effect on Performance Measures.” 2007 IEEE 8th Human Factors and Power Plants and HPRCT 13th Annual Meeting (2007): n. pag
- Koslowsky, Meni, and Harvey Babkoff. “Meta-Analysis of the Relationship Between Total Sleep Deprivation and Performance.” Chronobiology International 9.2 (1992): 132-36
- Wesensten, Nancy. “Effects of Modafinil on Cognitive Performance and Alertness During Sleep Deprivation.” CPD Current Pharmaceutical Design12.20 (2006): 2457-471
- Wesensten, Nancy, Gregory Belenky, Mary A. Kautz, David R. Thorne, Rebecca M. Reichardt, and Thomas J. Balkin. “Maintaining Alertness and Performance during Sleep Deprivation: Modafinil versus Caffeine.”Psychopharmacology 159.3 (2001): 238-47
- Wesensten, Nancy J., William D. S. Killgore, and Thomas J. Balkin. “Performance and Alertness Effects of Caffeine, Dextroamphetamine, and Modafinil during Sleep Deprivation.” Journal of Sleep Research J Sleep Res 14.3 (2005): 255-66
- Baranski, Joseph V., Corinne Cian, Dominique Esquivié, Ross A. Pigeau, and Christian Raphel. “Modafinil during 64 Hr of Sleep Deprivation: Dose-related Effects on Fatigue, Alertness, and Cognitive Performance.”Military Psychology 10.3 (1998): 173-93.
- Buguet, A., A. Montmayeur, R. Pigeau, and P. Naitoh. “Modafinil, D-amphetamine and Placebo during 64 Hours of Sustained Mental Work. II. Effects on Two Nights of Recovery Sleep.” Journal of Sleep Research 4.4 (1995): 229-41
- Pigeau, R., P. Naitoh, A. Buguet, C. Mccann, J. Baranski, M. Taylor, M. Thompson, and I. Mack. “Modafinil, D-amphetamine and Placebo during 64 Hours of Sustained Mental Work. I. Effects on Mood, Fatigue, Cognitive Performance and Body Temperature.” Journal of Sleep Research 4.4 (1995): 212-28
- Young, Jared W., and Mark A. Geyer. “Action of Modafinil—Increased Motivation Via the Dopamine Transporter Inhibition and D1 Receptors?“Biological Psychiatry 67.8 (2010): 784-87
- Volkow, Nora D. et al. “Effects of Modafinil on Dopamine and Dopamine Transporters in the Male Human Brain: Clinical Implications.” JAMA : the journal of the American Medical Association 301.11 (2009): 1148–1154. PMC. Web. 1 Sept. 2016.
- Taneja I, Haman K, Shelton RC, Robertson D. A randomized, double-blind, crossover trial of modafinil on mood. J Clin Psychopharmacol. 2007 Feb;27(1):76-9. PubMed PMID: 17224718
- Thase ME, Fava M, DeBattista C, Arora S, Hughes RJ. Modafinil augmentation of SSRI therapy in patients with major depressive disorder and excessive sleepiness and fatigue: a 12-week, open-label, extension study. CNS Spectr. 2006 Feb;11(2):93-102. PubMed PMID: 16520686
- Fava M, Thase ME, DeBattista C. A multicenter, placebo-controlled study of modafinil augmentation in partial responders to selective serotonin reuptake inhibitors with persistent fatigue and sleepiness. J Clin Psychiatry. 2005 Jan;66(1):85-93. PubMed PMID: 15669893
- Ninan PT, Hassman HA, Glass SJ, McManus FC. Adjunctive modafinil at initiation of treatment with a selective serotonin reuptake inhibitor enhances the degree and onset of therapeutic effects in patients with major depressive disorder and fatigue. J Clin Psychiatry. 2004 Mar;65(3):414-20. PubMed PMID: 15096082
- Konuk N, Atasoy N, Atik L, Akay O. Open-label study of adjunct modafinil for the treatment of patients with fatigue, sleepiness, and major depression treated with selective serotonin reuptake inhibitors. Adv Ther. 2006 Jul-Aug;23(4):646-54. PubMed PMID: 17050507
- Dunlop BW, Crits-Christoph P, Evans DL, Hirschowitz J, Solvason HB, Rickels K, Garlow SJ, Gallop RJ, Ninan PT.Coadministration of modafinil and a selective serotonin reuptake inhibitor from the initiation of treatment of major depressive disorder with fatigue and sleepiness: a double-blind, placebo-controlled study. J Clin Psychopharmacol. 2007 Dec;27(6):614-9. PubMed PMID: 18004129
- Menza, Matthew A., Kenneth R. Kaufman, and Ana Marietta Castellanos. “Modafinil Augmentation of Antidepressant Treatment in Depression.” J. Clin. Psychiatry The Journal of Clinical Psychiatry 61.5 (2000): 378-81
- Debattista, Charles, Anna Lembke, H. Brent Solvason, Rahwa Ghebremichael, and Jennifer Poirier. “A Prospective Trial of Modafinil as an Adjunctive Treatment of Major Depression.” Journal of Clinical Psychopharmacology 24.1 (2004): 87-90
- Abolfazli, Roya, Mahdi Hosseini, Ahmad Ghanizadeh, Ali Ghaleiha, Mina Tabrizi, Maedeh Raznahan, Mousa Golalizadeh, and Shahin Akhondzadeh. “Double-blind Randomized Parallel-group Clinical Trial of Efficacy of the Combination Fluoxetine plus Modafinil versus Fluoxetine plus Placebo in the Treatment of Major Depression.” Depression and Anxiety Depress. Anxiety 28.4 (2011): 297-302
- Goss, Alexander J., Muzaffer Kaser, Sergi G. Costafreda, Barbara J. Sahakian, and Cynthia H. Y. Fu. “Modafinil Augmentation Therapy in Unipolar and Bipolar Depression.” J. Clin. Psychiatry The Journal of Clinical Psychiatry 74.11 (2013): 1101-107
- Ballenger, J.c. “A Placebo-Controlled Evaluation of Adjunctive Modafinil in the Treatment of Bipolar Depression.” Yearbook of Psychiatry and Applied Mental Health 2009 (2009): 225
- Calabrese, Joseph R., Mark A. Frye, Ronghua Yang, and Terence A. Ketter. “Efficacy and Safety of Adjunctive Armodafinil in Adults With Major Depressive Episodes Associated With Bipolar I Disorder.” J. Clin. Psychiatry The Journal of Clinical Psychiatry (2014): 1054-061
- Ketter, Terence A., Ronghua Yang, and Mark A. Frye. “Adjunctive Armodafinil for Major Depressive Episodes Associated with Bipolar I Disorder.“Journal of Affective Disorders 181 (2015): 87-91
- Vaishnavi, Sandeep, Kishore Gadde, Sayed Alamy, Wei Zhang, Kathryn Connor, and Jonathan R.t. Davidson. “Modafinil for atypical depression: effects of open-label and double-blind discontinuation treatment.”Journal of Clinical Psychopharmacology 26.4 (2006): 373-78
- Randall, Delia C., John M. Shneerson, Komal K. Plaha, and Sandra E. File. “Modafinil Affects Mood, but Not Cognitive Function, in Healthy Young Volunteers.” Human Psychopharmacology: Clinical and Experimental Hum. Psychopharmacol. Clin. Exp. 18.3 (2003): 163-73
- Volkow, Nora D. et al. “Effects of Modafinil on Dopamine and Dopamine Transporters in the Male Human Brain: Clinical Implications.” JAMA : the journal of the American Medical Association 301.11 (2009): 1148–1154. PMC
- Dackis, Charles A., Kevin G. Lynch, Elmer Yu, Frederick F. Samaha, Kyle M. Kampman, James W. Cornish, Amy Rowan, Sabrina Poole, Lenae White, and Charles P. O’brien. “Modafinil and Cocaine: A Double-blind, Placebo-controlled Drug Interaction Study.” Drug and Alcohol Dependence 70.1 (2003): 29-37
- Verrico, Christopher D., Colin N. Haile, James J. Mahoney Iii, Daisy G.y. Thompson-Lake, Thomas F. Newton, and Richard De La Garza Ii. “Treatment with Modafinil and Escitalopram, Alone and in Combination, on Cocaine-induced Effects: A Randomized, Double Blind, Placebo-controlled Human Laboratory Study.” Drug and Alcohol Dependence 141 (2014): 72-78
- Kampman, Kyle M., Kevin G. Lynch, Helen M. Pettinati, Kelly Spratt, Michael R. Wierzbicki, Charles Dackis, and Charles P. O’Brien. “A Double Blind, Placebo Controlled Trial of Modafinil for the Treatment of Cocaine Dependence without Co-morbid Alcohol Dependence.” Drug and Alcohol Dependence 155 (2015): 105-10
- Dackis, Charles A., Kyle M. Kampman, Kevin G. Lynch, Helen M. Pettinati, and Charles P. O’brien. “A Double-Blind, Placebo-Controlled Trial of Modafinil for Cocaine Dependence.” Neuropsychopharmacology 30.1 (2004): 205-11
- Boivin, D. B., J. Montplaisir, D. Petit, C. Lambert, and S. Lubin. “Effects of Modafinil on Symptomatology of Human Narcolepsy.” Clinical Neuropharmacology 16.1 (1993): 46-53
- Hou, R. H., C. Freeman, R. W. Langley, E. Szabadi, and C. M. Bradshaw. “Does Modafinil Activate the Locus Coeruleus in Man? Comparison of Modafinil and Clonidine on Arousal and Autonomic Functions in Human Volunteers.” Psychopharmacology 181.3 (2005): 537-49
- Minzenberg, M. J., A. J. Watrous, J. H. Yoon, S. Ursu, and C. S. Carter. “Modafinil Shifts Human Locus Coeruleus to Low-Tonic, High-Phasic Activity During Functional MRI.” Science 322.5908 (2008): 1700-702
- Winder-Rhodes, Se et al. “Effects of Modafinil and Prazosin on Cognitive and Physiological Functions in Healthy Volunteers.”Pharmacopsychiatry, vol. 42, no. 05, 2009
- Vosburg, Suzanne K. et al. “Modafinil Does Not Serve as a Reinforcer in Cocaine Abusers.” Drug and Alcohol Dependence, vol. 106, no. 2-3, 2010, pp. 233–236. doi:10.1016/j.drugalcdep.2009.09.002
- MuLler, Ulrich et al. “Effects of Modafinil on Working Memory Processes in Humans.” Psychopharmacology, vol. 177, no. 1-2, 2004, pp. 161–169. doi:10.1007/s00213-004-1926-3.
- Samuels, E. R. et al. “Comparison of Pramipexole and Modafinil on Arousal, Autonomic, and Endocrine Functions in Healthy Volunteers.” Journal of Psychopharmacology, vol. 20, no. 6, Sept. 2006, pp. 756–770. doi:10.1177/0269881106060770
- Brun, Jocelyne et al. “Effect of Modafinil on Plasma Melatonin, Cortisol and Growth Hormone Rhythms, Rectal Temperature and Performance in Healthy Subjects during a 36 h Sleep Deprivation.” Journal of Sleep Research, vol. 7, no. 2, 1998, pp. 105–114. doi:10.1046/j.1365-2869.1998.00100.x.
- Repantis, Dimitris et al. “Modafinil and Methylphenidate for Neuroenhancement in Healthy Individuals: A Systematic Review.”Pharmacological Research, vol. 62, no. 3, 2010, pp. 187–206. doi:10.1016/j.phrs.2010.04.002.
- Samuels, Ebony R et al. “Modulation of the Acoustic Startle Response by the Level of Arousal: Comparison of Clonidine and Modafinil in Healthy Volunteers.” Neuropsychopharmacology, vol. 32, no. 11, July 2007, pp. 2405–2421. doi:10.1038/sj.npp.1301363
- Lundt, L. “Modafinil Treatment in Patients with Seasonal Affective Disorder/Winter Depression: an Open-Label Pilot Study.” Journal of Affective Disorders, vol. 81, no. 2, 2004, pp. 173–178. doi:10.1016/s0165-0327(03)00162-9.
- Debattista, Charles et al. “Adjunct Modafinil for the Short-Term Treatment of Fatigue and Sleepiness in Patients With Major Depressive Disorder.” J. Clin. Psychiatry The Journal of Clinical Psychiatry, vol. 64, no. 9, 2003, pp. 1057–1064. doi:10.4088/jcp.v64n0911.
- Subjective effects of modafinil, a new central adrenergic stimulant in healthy volunteers: A comparison with amphetamine, caffeine and placebo. Warot, D.; Corruble, E.; Payan, C.; Weil, J. S.; et al European Psychiatry, Vol 8(4), 1993, 201-208
- Ferraro, Luca et al. “Modafinil: An Antinarcoleptic Drug with a Different Neurochemical Profile to d-Amphetamine and Dopamine Uptake Blockers.” Biological Psychiatry, vol. 42, no. 12, 1997, pp. 1181–1183. doi:10.1016/s0006-3223(97)00353-3.
- Spathis, A. et al. “Modafinil for the Treatment of Fatigue in Lung Cancer: a Pilot Study.” Lung Cancer, vol. 60, 2008, doi:10.1016/s0169-5002(08)70013-8.
- Morrow, G. R., Gillies, L. J., Hickok, J. T., Roscoe, J. A., Padmanaban, D., Griggs, J. J. “The positive effect of the psychostimulant modafinil on fatigue from cancer that persists after treatment is completed” J Clin Oncol (Meeting Abstracts) 2005 23: 8012
- Davis, Mellar. “Faculty of 1000 Evaluation for Modafinil for the Treatment of Fatigue in Lung Cancer: Results of a Placebo-Controlled, Double-Blind, Randomized Trial.” F1000 – Post-Publication Peer Review of the Biomedical Literature, doi:10.3410/f.718365592.793498273.
- Rabkin, J. G. et al. “Modafinil and Armodafinil Treatment for Fatigue for HIV-Positive Patients with and without Chronic Hepatitis C.” International Journal of STD &Amp; AIDS, vol. 22, no. 2, Jan. 2011, pp. 95–101. doi:10.1258/ijsa.2010.010326.
- Rabkin, Judith G. et al. “Modafinil Treatment for Fatigue in HIV Patients.” J. Clin. Psychiatry The Journal of Clinical Psychiatry, vol. 65, no. 12, 2004, pp. 1688–1695. doi:10.4088/jcp.v65n1215.
- Gordon, M.s. “Modafinil Treatment for Fatigue in HIV/AIDS: A Randomized Placebo-Controlled Study.” Yearbook of Oncology, vol. 2010, 2010, pp. 4–5. doi:10.1016/s1040-1741(10)79566-x.
- Bodenmann, S et al. “Pharmacogenetics of Modafinil After Sleep Loss: Catechol-O-Methyltransferase Genotype Modulates Waking Functions But Not Recovery Sleep.” Clin Pharmacol Ther Clinical Pharmacology &Amp; Therapeutics, vol. 85, no. 3, 2008, pp. 296–304. doi:10.1038/clpt.2008.222
- Kim, Woochan et al. “In Vivo Activity of Modafinil on Dopamine Transporter Measured with Positron Emission Tomography and [18F]FE-PE2I.” The International Journal of Neuropsychopharmacology Int. J. Neuropsychopharm., vol. 17, no. 05, 2014, pp. 697–703. doi:10.1017/s1461145713001612.
- Makris, Angela P. et al. “Behavioral and Subjective Effects of D-Amphetamine and Modafinil in Healthy Adults.” Experimental and Clinical Psychopharmacology, vol. 15, no. 2, 2007, pp. 123–133. doi:10.1037/1064-1297.15.2.123
- Taylor, Fletcher B., and Joan Russo. “Efficacy of Modafinil Compared to Dextroamphetamine for the Treatment of Attention Deficit Hyperactivity Disorder in Adults.” Journal of Child and Adolescent Psychopharmacology, vol. 10, no. 4, 2000, pp. 311–320. doi:10.1089/cap.2000.10.311.
- Greenhill, Laurence L. et al. “A Randomized, Double-Blind, Placebo-Controlled Study of Modafinil Film-Coated Tablets in Children and Adolescents With Attention-Deficit/Hyperactivity Disorder.” Journal of the American Academy of Child &Amp; Adolescent Psychiatry, PAP, 2006, doi:10.1097/01.chi.0000205709.63571.
- Biederman, J. et al. “Efficacy and Safety of Modafinil Film-Coated Tablets in Children and Adolescents With Attention-Deficit/Hyperactivity Disorder: Results of a Randomized, Double-Blind, Placebo-Controlled, Flexible-Dose Study.” Pediatrics, vol. 116, no. 6, Jan. 2005, doi:10.1542/peds.2005-0617.
- Kahbazi, Manijeh et al. “A Randomized, Double-Blind and Placebo-Controlled Trial of Modafinil in Children and Adolescents with Attention Deficit and Hyperactivity Disorder.” Psychiatry Research, vol. 168, no. 3, 2009, pp. 234–237. doi:10.1016/j.psychres.2008.06.024.
- Swanson, James M. et al. “Modafinil Film-Coated Tablets in Children and Adolescents With Attention-Deficit/Hyperactivity Disorder: Results of a Randomized, Double-Blind, Placebo-Controlled, Fixed-Dose Study Followed by Abrupt Discontinuation.” J. Clin. Psychiatry The Journal of Clinical Psychiatry, vol. 67, no. 01, 2006, pp. 137–147. doi:10.4088/jcp.v67n0120.
- Biederman, Joseph et al. “A Comparison of Once-Daily and Divided Doses of Modafinil in Children with Attention-Deficit/Hyperactivity Disorder: a Randomized, Double-Blind, and Placebo-Controlled Study.” J. Clin. Psychiatry The Journal of Clinical Psychiatry, vol. 67, no. 05, 2006, pp. 727–735. doi:10.4088/jcp.v67n0506.
- Rasmussen, Niels-Anton et al. “Modafinil Augmentation in Depressed Patients with Partial Response to Antidepressants: A Pilot Study on Self-Reported Symptoms Covered by the Major Depression Inventory (MDI) and the Symptom Checklist (SCL-92).” Nordic Journal of Psychiatry, vol. 59, no. 3, 2005, pp. 173–178
- Wisor JP, Nishino S, Sora I, Uhl GH, Mignot E, Edgar DM. Dopaminergic role in stimulant-induced wakefulness. J Neurosci. 2001 Mar 1;21(5):1787-94. PubMed PMID: 11222668
- Qu, W.-M. et al. “Dopaminergic D1 and D2 Receptors Are Essential for the Arousal Effect of Modafinil.” Journal of Neuroscience, vol. 28, no. 34, 2008, pp. 8462–8469. doi:10.1523/jneurosci.1819-08.2008.
- Wisor, J.p., and K.s. Eriksson. “Dopaminergic—Adrenergic Interactions in the Wake Promoting Mechanism of Modafinil.” Neuroscience, vol. 132, no. 4, 2005, pp. 1027–1034. doi:10.1016/j.neuroscience.2005.02.003.
- Dopheide, Marsha M. et al. “Modafinil Evokes Striatal [3H]Dopamine Release and Alters the Subjective Properties of Stimulants.” European Journal of Pharmacology, vol. 568, no. 1-3, 2007, pp. 112–123. doi:10.1016/j.ejphar.2007.03.044
- Hilaire, Zara De Saint et al. “Variations in Extracellular Monoamines in the Prefrontal Cortex and Medial Hypothalamus after Modafinil Administration: a Microdialysis Study in Rats.” Neuroreport, vol. 12, no. 16, 2001, pp. 3533–3537.
- Madras, B. K. et al. “Modafinil Occupies Dopamine and Norepinephrine Transporters in Vivo and Modulates the Transporters and Trace Amine Activity in Vitro.” Journal of Pharmacology and Experimental Therapeutics, vol. 319, no. 2, 2006, pp. 561–569. doi:10.1124/jpet.106.106583.
- Akaoka, Hidéo et al. “Effect of Modafinil and Amphetamine on the Rat Catecholaminergic Neuron Activity.” Neuroscience Letters, vol. 123, no. 1, 1991, pp. 20–22. doi:10.1016/0304-3940(91)90148-m.
- Lin, J.s. et al. “Role of Catecholamines in the Modafinil and Amphetamine Induced Wakefulness, a Comparative Pharmacological Study in the Cat.” Brain Research, vol. 591, no. 2, 1992, pp. 319–326. doi:10.1016/0006-8993(92)91713-o.
- Duteil, Jacques et al. “Central α1-Adrenergic Stimulation in Relation to the Behaviour Stimulating Effect of Modafinil; Studies with Experimental Animals.” European Journal of Pharmacology, vol. 180, no. 1, 1990, pp. 49–58. doi:10.1016/0014-2999(90)90591-s
- Tanganelli, S. et al. “Inhibitory Effects of the Psychoactive Drug Modafinil on ?-Aminobutyric Acid Outflow from the Cerebral Cortex of the Awake Freely Moving Guinea-Pig.” Naunyn-Schmiedeberg’s Archives of Pharmacology Naunyn-Schmiedeberg’s Arch Pharmacol, vol. 345, no. 4, 1992, doi:10.1007/bf00176625.
- Ferraro, Luca et al. “The Vigilance Promoting Drug Modafinil Decreases GABA Release in the Medial Preoptic Area and in the Posterior Hypothalamus of the Awake Rat: Possible Involvement of the Serotonergic 5-HT3 Receptor.” Neuroscience Letters, vol. 220, no. 1, 1996, pp. 5–8. doi:10.1016/s0304-3940(96)13212-2.
- Tanganelli, Sergio et al. “6-Hydroxy-Dopamine Treatment Counteracts the Reduction of Cortical GABA Release Produced by the Vigilance Promoting Drug Modafinil in the Awake Freely Moving Guinea-Pig.” Neuroscience Letters, vol. 171, no. 1-2, 1994, pp. 201–204. doi:10.1016/0304-3940(94)90639-4.
- Tanganelli, Sergio et al. “Modafinil and Cortical γ-Aminobutyric Acid Outflow. Modulation by 5-Hydroxytryptamine Neurotoxins.” European Journal of Pharmacology, vol. 273, no. 1-2, 1995, pp. 63–71. doi:10.1016/0014-2999(94)00675-w.
- Ferraro, Luca et al. “The Vigilance Promoting Drug Modafinil Increases Dopamine Release in the Rat Nucleus Accumbens via the Involvement of a Local GABAergic Mechanism.” European Journal of Pharmacology, vol. 306, no. 1-3, 1996, pp. 33–39. doi:10.1016/0014-2999(96)00182-3.
- Mora, Miguel Pérez De La et al. “Effects of the Vigilance Promoting Drug Modafinil on the Synthesis of GABA and Glutamate in Slices of Rat Hypothalamus.” Neuroscience Letters, vol. 259, no. 3, 1999, pp. 181–185. doi:10.1016/s0304-3940(98)00905-7.
- Ferraro, L. “The Vigilance Promoting Drug Modafinil Increases Extracellular Glutamate Levels in the Medial Preoptic Area and the Posterior Hypothalamus of the Conscious Rat Prevention by Local GABAA Receptor Blockade.” Neuropsychopharmacology, vol. 20, no. 4, 1999, pp. 346–356. doi:10.1016/s0893-133x(98)00085-2.
- Ishizuka, Tomoko et al. “Modafinil Increases Histamine Release in the Anterior Hypothalamus of Rats.” Neuroscience Letters, vol. 339, no. 2, 2003, pp. 143–146. doi:10.1016/s0304-3940(03)00006-5.
- Ishizuka, Tomoko et al. “Action of Modafinil Through Histaminergic and Orexinergic Neurons.” Sleep Hormones Vitamins &Amp; Hormones, 2012, pp. 259–278. doi:10.1016/b978-0-12-394623-2.00014-7.
- Lin, Jian-Sheng et al. “An Inverse Agonist of the Histamine H3 Receptor Improves Wakefulness in Narcolepsy: Studies in Orexin−/− Mice and Patients.” Neurobiology of Disease, vol. 30, no. 1, 2008, pp. 74–83. doi:10.1016/j.nbd.2007.12.003.
- Willie, J.t. et al. “Modafinil More Effectively Induces Wakefulness in Orexin-Null Mice than in Wild-Type Littermates.” Neuroscience, vol. 130, no. 4, 2005, pp. 983–995. doi:10.1016/j.neuroscience.2004.10.005.
- Battleday, R.m., and A.-K. Brem. “Modafinil for Cognitive Neuroenhancement in Healthy Non-Sleep-Deprived Subjects: A Systematic Review.” European Neuropsychopharmacology, vol. 26, no. 2, 2016, p. 391. doi:10.1016/j.euroneuro.2015.12.023
- Saletu B, Frey R, Krupka M, Anderer P, Grünberger J, Barbanoj MJ. Differential effects of a new central adrenergic agonist–modafinil–and D-amphetamine on sleep and early morning behaviour in young healthy volunteers. Int J Clin Pharmacol Res. 1989;9(3):183-95. PubMed PMID: 2568348.
- Lyons TJ, French J. Modafinil: the unique properties of a new stimulant. Aviat Space Environ Med. 1991 May;62(5):432-5. PubMed PMID: 1675850
- Robertson, Philmore, and Edward T. Hellriegel. “Clinical Pharmacokinetic Profile of Modafinil.” Clinical Pharmacokinetics, vol. 42, no. 2, 2003, pp. 123–137. doi:10.2165/00003088-200342020-00002.
- Mitler, Merrill M et al. “Long-Term Efficacy and Safety of Modafinil (PROVIGIL®) for the Treatment of Excessive Daytime Sleepiness Associated with Narcolepsy.” Sleep Medicine, vol. 1, no. 3, 2000, pp. 231–243. doi:10.1016/s1389-9457(00)00031-9
- Wong, Y. Nancy et al. “A Double-Blind, Placebo-Controlled, Ascending-Dose Evaluation of the Pharmacokinetics and Tolerability of Modafinil Tablets in Healthy Male Volunteers.” The Journal of Clinical Pharmacology, vol. 39, no. 1, 1999, pp. 30–40. doi:10.1177/00912709922007534
- Wong, Y. Nancy et al. “Comparison of the Single-Dose Pharmacokinetics and Tolerability of Modafinil and Dextroamphetamine Administered Alone or in Combination in Healthy Male Volunteers.” The Journal of Clinical Pharmacology, vol. 38, no. 10, 1998, pp. 971–978. doi:10.1002/j.1552-4604.1998.tb04395.x.
- Clemons, William Eric et al. “Concomitant Use of Modafinil and Tranylcypromine in a Patient with Narcolepsy: a Case Report.” Sleep Medicine, vol. 5, no. 5, 2004, pp. 509–511. doi:10.1016/j.sleep.2004.06.006.
- Amar, Jacques et al. “Arterial Hypertension and Resistance to Antihypertensive Treatment: a New Adverse Drug Reaction with Modafinil.” Thérapie, vol. 68, no. 1, 2013, pp. 53–54. doi:10.2515/therapie/2013007.
- EH, Tobe. “Modafinil Enhances Two-Year Outcome from Monoamine Oxidase Inhibitor Therapy in 3 Patients with Treatment-Resistant Depression.”Advances in Pharmacoepidemiology &Amp; Drug Safety Adv Pharmacoepidemiol Drug Saf, vol. 04, no. 04, 2015, doi:10.4172/2167-1052.1000189.
- Ferraro, Luca et al. “Modafinil: An Antinarcoleptic Drug with a Different Neurochemical Profile to d-Amphetamine and Dopamine Uptake Blockers.” Biological Psychiatry, vol. 42, no. 12, 1997, pp. 1181–1183. doi:10.1016/s0006-3223(97)00353-3.
- Robertson, Philmore et al. “Effect of Modafinil at Steady State on the Single-Dose Pharmacokinetic Profile of Warfarin in Healthy Volunteers.” The Journal of Clinical Pharmacology, vol. 42, no. 2, 2002, pp. 205–214. doi:10.1177/00912700222011120.
Does Modafinil show up in urine tests..My employer wants to start drug tests for the ice addicts etc..
If they’re testing for Modafinil then yes it will show up in the urine test. By ice addicts I’m assuming you’re referring to methamphetamine, eh? If so, it’s highly unlikely that modafinil will trigger a false positive for meth.
I started taking 200mg of Modafinil 3 days ago to help me with fatigue. It only helps for 2 to 4 hours. I was taking Oxycodone & Morphine for the last 4 years for chronic neck & back pain. I did stop taking these pain meds about 5 years ago & within a day or two regained my energy. I only took them for about 8 months at that time. Now after taking them for 4 years & stopping about 2 months ago , because I would rather have pain than the side effects & the dependence on them. When I stopped I had no energy & still don’t. I lost about 30lb. The last 2 months . Just because I have no energy to get up & eat. I tried everything to get more energy. Now Modafinil. Any suggestions to discuss with my Doctor. Or should I just give Modafinil more time to work. I’m 6’4″ and weigh 205 now after losing 30lb. I’m eating better this week as I know I need food for energy. I was reading that it could take 6 months or more to regain my energy after stopping the pain meds. I can’t wait that long. I feel the fatigue in every muscle of my body. Any suggestions would be appreciated. Thanks for your time.
Hi Paul, sorry to hear that modafinil isn’t working well for you. Typically, modafinil works immediately for fatigue. So I don’t think its effects will improve with time. There are quite a few things I’d try to improve your response.
First, you could try a high quality multivitamin like Life Extension two per day (I’d take 1 capsule/tablet though). This just ensures that your body is getting all the nutrients it needs, so it may or may not be helpful, depending on your diet.
Second, ask your doctor to test your iron and vitamin B12 levels. If your ferritin levels are below 50 ng/dl then you may not have adequate dopamine production. There’s a direct link between iron levels and dopamine-deficient illnesses like ADHD and restless leg syndrome. You don’t have to have anemia for it to have an effect on your dopamine system.
See these studies: https://jamanetwork.com/journals/jamapediatrics/fullarticle/485884
https://pubmed.ncbi.nlm.nih.gov/17984624/
Though, be careful with iron as it can become toxic if you take it for too long. Ask your doctor about this.
But vitamin B12 is non-toxic even at high doses. I’d recommend trying adenosylcobalamin, which is an active form of B12 that mainly helps with energy. It might be hard to find in store, but iHerb carries: https://iherb.com/search?kw=adenosylcobalamin
You can use my affiliate code to get a discount: JAF208.
Also, you might want to consider methylfolate. Some people have had life changing effects from it.
Fatigue is a common symptom among those with non-optimal methylation. Unfortunately, the science behind it is still lacking so you’ll have to experiment on your own.
Third, I’d recommend you start taking agmatine to help upregulate your opioid receptors. Agmatine is quite helpful for reducing opioid dependence: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2923207/
But I think it’ll also be helpful even if you don’t take an opioid. It might reduce the time needed to balance your opioid system after stopping those meds.
Another thing you can try is Rhodiola Rosea. It’s a herb that’s known for its anti-fatigue effects. Plus, it increases beta-endorphin, one of the body’s natural opioid.
In terms of medication, I know of 2 things you can try: Low-dose naltrexone or low-dose Selegiline.
For the former, it’s mainly to reduce the withdrawal from the opioids you used to take.
For the latter, it’s to augment the effects of modafinil. In this case, it might take about 2-3 weeks before you notice any significant effects.
Lastly, Kratom is widely used as a substitute for opioids and there are strains that help with energy. But you should consider this option carefully as it may have some dependence, though not as severe as the drugs. Maybe you can take it to reduce your withdrawal symptoms and then ween off it?
So to sum it up:
• Take a high-quality multivitamin
• Check your iron and Vitamin B12 levels
• Try adenosylcobalamin and methylfolate
• Try Agmatine and Rhodiola Rosea
• Consider low-dose naltrexone or low-dose selegiline
• Kratom as an alternative to opioids
Let me know if this helps.